by Jack Norris, RD
Contents
- Introduction
- Brief History of B12 Recommendations for Vegans
- Government Recommendations
- Cyanocobalamin Absorption
- Vegan Health B12 Recommendations
- Appendix A. Minimizing Methylmalonic Acid Levels
- Appendix B. Clinical Trials: Impact of B12 Supplementation on Metabolites
- Serum B12
- Holotranscobalamin
- Methylmalonic Acid
- Homocysteine
- Notes on Clinical Trials of B12 Supplementation
- Appendix C. Factorial Approach
- Appendix D. Pregnancy and Breastfeeding
- Appendix E. IOM Recommendations for People Over Age 50
- Appendix F. ASMBS B12 Recommendations for People after Bariatric Surgery
- Appendix G. Taking Vitamin B12 With or Without Food
- Bibliography
Introduction
Vitamin B12 recommendations vary across countries. For the United States, the Institute of Medicine (IOM) has set a recommended dietary allowance (RDA) of 2.4 µg/day for adults; it also recommends that people over 50 receive half the RDA from fortified foods or supplements because that form of B12 is not bound to protein and is easier to absorb (IOM, 1998). The European Food Safety Authority (EFSA) has set an adequate intake (AI) of 4.0 µg/day for adults (EFSA, 2015).
Brief History of B12 Recommendations for Vegans
Government recommendations for B12 are created with the assumption that people receive multiple doses of B12 from foods throughout the day. In typical dietary doses, B12 is absorbed at a rate of about 40-50%.
Intrinsic factor, a protein that shuttles B12 through the absorption process, becomes saturated after a meal containing an above-average amount of B12 and about 4 to 6 hours are required before it can efficiently absorb another dose (IOM, 1998). However, a very small percentage of B12 from a supplemental dose is absorbed by passive diffusion, rather than by intrinsic factor, such that vegans can make up for taking B12 only once per day, or even only once per week, by taking larger doses than normally provided by food. B12-fortified foods are available in many countries, but for convenience and reliability, recommendations for vegans have focused on supplements.
In the years immediately following the IOM’s 1998 report setting the current RDA, research associated an abnormally high level of homocysteine, a molecule involved in protein metabolism, with an increased risk of cardiovascular disease, mortality, and cognitive impairment. Homocysteine levels tend to be higher in people who don’t have adequate folate and B12 intakes.
Vegetarians and vegans generally have higher intakes of folate than omnivores, making them an interesting group to study with regard to homocysteine. Many studies found that vegans who didn’t supplement with B12 generally had high homocysteine levels. For this reason, our 2001 B12 recommendations in What Every Vegan Should Know about Vitamin B12 were focused as much on keeping homocysteine levels low as on preventing the traditional B12 deficiency symptoms of blood and nerve abnormalities.
Since 2001, many clinical trials have been conducted on omnivores to see if lowering homocysteine through pharmacological doses of folate, B12, and sometimes vitamin B6, could reduce the risk of cardiovascular disease, premature death, and cognitive decline. The trials failed to show much benefit, though there appears to be a small protection against stroke and possibly cognitive decline. For more details, see our article Homocysteine and Mild B12 Deficiency in Vegans. Because of the disappointing results of clinical trials, minimizing homocysteine levels is no longer the primary goal of our recommendations.
Unlike homocysteine, which responds to both B12 and folate intake, the metabolite methylmalonic acid (MMA) specifically responds to B12 intake, and for some time we viewed MMA levels as the most important measure of B12 activity. When it was discovered that very high doses of B12 were required for older adults to minimize their MMA levels, we raised our recommendations for older adults. But using MMA levels to determine B12 status has its own complications. There’s been no research to determine optimal MMA levels, and usual levels appear to have a wide range and to increase with age. While supplementing with large doses of B12 will reduce MMA levels more than will smaller doses, there are no clear benefits (more info in Appendix A. Minimizing Methylmalonic Acid Levels).
Pawlak and others reviewed studies of B12 deficiency among vegetarians and vegans using serum B12 (Pawlak, 2014) as well as methylmalonic acid and holotranscobalamin (Pawlak, 2013); symptoms were not assessed. They found a high rate of deficiency based on typical reference ranges and determined that it doesn’t require 20 to 30 years of being vegetarian to develop a deficiency, a popular belief among vegetarians (Pawlak, 2013). With only a brief analysis of B12 requirements, they recommend vegetarians take a supplement of 250 µg per day (Pawlak, 2013).
In 2015, the EFSA released B12 recommendations that considers the research published since the 1998 IOM’s recommendations (EFSA, 2015; IOM, 1998). Our B12 recommendations are now geared towards matching those of the EFSA.
Government Recommendations
In this section, we’ll examine the main rationale behind the IOM and EFSA recommendations.
Institute of Medicine’s Recommendations
In their 1998 report, the IOM used the amount of B12 required to treat pernicious anemia as a basis for their recommendations for the general adult population (IOM, 1998).
Pernicious anemia is an autoimmune disease in which the immune system attacks the parietal cells of the stomach which produce intrinsic factor, a protein normally responsible for most of the body’s B12 absorption. Analyzing a series of studies using differing amounts of B12 via injection, the IOM determined that 1.5 µg of absorbed B12 per day was enough to normalize red blood cell parameters (hematocrit, red blood cell volume, and anemia) in the average patient with pernicious anemia. In people without pernicious anemia, about 0.5 µg/day of B12 is reabsorbed by enterohepatic circulation in which B12-containing bile is secreted by the liver into the digestive tract where the B12 is then reabsorbed via intrinsic factor. Subtracting this 0.5 µg of reabsorbed B12 from the 1.5 µg that normalizes blood parameters results in a requirement of 1.0 µg absorbed per day (for those without pernicious anemia). The IOM then doubled the amount because only about 50% of dietary B12 is absorbed, and arrived at an estimated average requirement (EAR) of 2.0 µg. They then increased the EAR by 20% to arrive at an RDA of 2.4 µg which aims to cover the needs of 97% to 98% of the population. Thus, the RDA assumes an absorbed amount of 1.2 µg per day (50% of 2.4 µg) or 8.4 µg per week.
Average B12 Intakes in the U.S.
The B12 intake for most Americans is well above the RDA. A report from the Framingham Offspring Study of 2,999 adults found the following average daily B12 intakes, including fortified foods and supplements (Tucker, 2000):
- Age 26-49: 8.9 µg
- Age 50-64: 8.7 µg
- Age 65-83: 8.5 µg
A 2015-2016 National Health and Nutrition Examination Survey of over 4,500 adults 60 years and older found the following average daily B12 intakes (USDA NHANES, 2019):
- Male non-supplement users (68% of men): 4.5 µg
- Male supplement users: 5.3 µg from food plus 326 µg from supplements
- Female non-supplement users (63% of women): 3.6 µg
- Female supplement users: 3.8 µg from food plus 520 µg from supplements
European Food Safety Authority’s Recommendations
In 2015, the EFSA released recommendations for B12 intake across Europe. In so doing, they reviewed the recommendations of eight international panels whose daily recommendations for adults ranged from 1.5 µg to 3.0 µg (EFSA, 2015).
While the IOM had based B12 needs on the amount required to correct hematological parameters for people with pernicious anemia, the EFSA had almost 20 more years of research to draw on, and concluded that the most suitable approach was basing needs on biomarkers (serum B12, holotranscobalamin, MMA, and homocysteine). They found that it wasn’t possible to determine a clear lower limit for which any of these biomarkers can reliably indicate B12 deficiency, but that daily intakes above 4.0 µg appear to have no additional benefit. They compared a target of 4.0 µg/day against typical European intakes which range from 4.2 to 8.6 μg/day in adults and believed 4.0 µg/day to be a practical amount. Thus, the EFSA set an AI of 4.0 µg per day.
The EFSA concluded that there wasn’t enough data to directly create recommendations for children, and so they used an extrapolation from the adult recommendations based on body size and applied a factor for increased needs due to growth (EFSA, 2015, p. 37). For pregnancy and breastfeeding, the EFSA assumes an extra 0.2 µg and 0.4 µg of daily absorbed B12, respectively.
The EFSA bases their recommendations on intake, as distinct from the amount absorbed used by the IOM. For this reason, we based the target weekly absorption from EFSA by dividing their daily recommendations into three meals and applying a formula devised by Stephen Walsh of the UK Vegan Society (see Cyanocobalamin Absorption below). For adults, this results in 14.9 µg of B12 absorbed per week.
Cyanocobalamin Absorption
Cyanocobalamin is the most common form of oral supplemental B12; it’s the most stable form of B12 and, unlike other forms of oral supplemental B12, it’s been studied rigorously. If we know the amount of B12 absorbed from various supplemental doses of cyanocobalamin, we can create recommendations to meet the predicted amount of B12 absorbed per week by the IOM and EFSA recommendations.
At typical dietary doses, B12 is absorbed at a rate of about 40-50% by way of intrinsic factor. Additionally, a very small percentage of B12 from a supplemental dose is absorbed by passive diffusion. Because of these different pathways, the formula for B12 absorption is complex. Numerous studies have measured the absorption of cyanocobalamin at a range of doses and using a variety of methods. The largest dataset based on whole-body counting is provided by Heinrich (Heinrich, 1967), who studied doses up to 100,000 µg. Heinrich determined that a dose (D) of cyanocobalamin is absorbed at a rate of:
Stephen Walsh, PhD, a mathematical modeler associated with the UK Vegan Society, has analyzed Heinrich’s data and found this formula to be a better fit:
Heinrich’s data assumes that the cyanocobalamin is taken on an empty stomach. In order to adjust for a 40% reduced passive absorption for taking with food, Walsh’s equation above applies .005 (rather than .009) to the second half of the equation.
In the spreadsheet B12 Doses and Absorption, we provide the calculations for B12 regimens for vegans to meet the IOM’s RDA and the EFSA’s AI. Because the IOM’s RDA is considerably lower than the EFSA’s AI, we chose to provide a lower recommendation to meet the RDA and a higher recommendation to meet the EFSA’s AI. While there isn’t solid evidence that human requirements for B12 exceed the RDA, meeting the EFSA will put any vegan on par with most omnivores and should ensure optimal B12 status for anyone without suspected abnormal B12 metabolism.
Because the IOM bases the RDA on the absorbed amount of B12 necessary to prevent deficiency, it’s straightforward to calculate the IOM’s weekly target absorption. Because the EFSA bases their AI on dietary intake, we divided their daily recommendations by three, to represent three meals per day, and applied Walsh’s formula to determine the targeted weekly absorption. Once we had the weekly absorption, we reversed Walsh’s formula to determine the various regimens required to meet the targeted absorption (for both the AI and the RDA) and then rounded them to practical amounts.
For children, Walsh modified his formula taking into account B12 absorption amounts found in children by Hjelt and Krasilnikoff (Hjelt, 1986). We erred on the side of lower passive absorption for children and decided not to recommend doses less frequently than once per day for children up to 3 years of age.
Because cyanide is a component of cyanocobalamin, we calculated the maximum cyanide load from various B12 regimens in the Cyanide Load tab of B12 Doses and Absorption. All of our regimens will provide a physiologically negligible amount of cyanide well below the EFSA’s acute reference dose safety threshold of 20 µg/kg of body weight (1,270 µg for a 140 lb (63.5 kg) person) per day. For more information, see Vitamin B12 and Cyanide.
Vegan Health B12 Recommendations
The table below shows our cyanocobalamin recommendations for vegans to meet the IOM’s RDA and the EFSA’s AI for vitamin B12 (larger version in B12 Doses and Absorption).
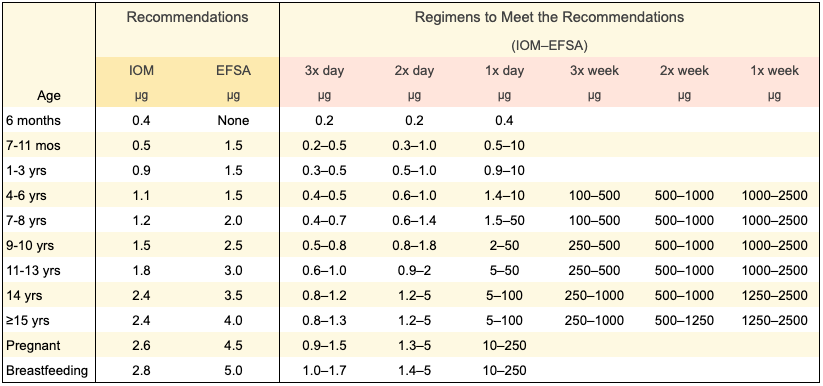
The amounts in the table are minimum amounts to meet the guidelines. While there’s no definite cutoff for when B12 starts to become unsafe, because people often ask, we’ll somewhat arbitrarily say not to take more than 1,000 µg per day over the long-term without guidance from a physician.
B12 tablets can often be cut in half or added together. As a rule, it’s going to be more economical to take smaller doses more often. For example, if your supplement happens to be 10 µg, then cutting it in half and taking the resulting 5 µg supplement twice a day (at least 4 hours apart) will meet the EFSA recommendations. But if you have a 500 µg supplement and only want to take B12 once a week, you can add 5 of them together to equal 2,500 µg and match our EFSA recommendation.
See Appendix D. Pregnancy and Breastfeeding for why we don’t recommend regimens less frequently than once per day during pregnancy and breastfeeding.
Note: If you’ve shown clinical symptoms of B12 deficiency or have a digestive condition that might cause malabsorption, talk to a doctor about a regimen tailored to best fit your situation.
People with Kidney Disease
About 38% of Americans ≥65 years old have chronic kidney disease (CDCP, 2019). Anyone with kidney disease should talk to their doctor about an appropriate B12 regimen. Following our recommendations will provide a minimal amount of cyanide, with the lowest amounts provided by the regimens on the left half of the Recommendations table above (i.e., smaller doses with more frequency).
Appendix A. Minimizing Methylmalonic Acid Levels
A potential problem with the IOM’s method for determining B12 requirements (see Institute of Medicine’s Recommendations above), is that a small percentage of people with neurological symptoms of B12 deficiency have normal blood parameters, including 13% of patients in one series of case studies (Lindenbaum, 1988). However, as described below, there doesn’t seem to be a benefit for neurological problems in going beyond the amount of B12 generally recommended by the EFSA.
An elevated methylmalonic acid (MMA) level has been thought to be the most direct, metabolic indicator of B12 deficiency because B12 is the only cofactor required by the enzyme that degrades MMA. Research consistently shows an inverse association between serum B12 and serum MMA levels, although researchers haven’t found specific cutoff points for determining B12 deficiency by way of serum B12 or MMA levels using cross-sectional data (Bailey, 2011, Bailey, 2013). As serum B12 levels drop below what’s considered deficient, MMA levels start to increase more drastically (Clarke, 2003). Normal serum MMA levels are typically thought to be less than 270 nmol/l in apparently healthy people, but there’s little evidence of direct harm for amounts even twice as high as 270 nmol/l.
A Danish research group produced a series of reports examining MMA levels in people suspected of mild B12 deficiency. In their initial study of 403 patients, the median MMA measurement was 330 nmol/l. The average patient age was 75 years (range: 23 to 102 years). While age was associated with clinical symptoms, there was very little association between MMA levels and other biochemical parameters or clinical symptoms, including neurological symptoms. No significant difference in the prevalence of symptoms was found between participants with MMA levels ≥400 nmol/l (n = 60) and those whose levels were < 400 nmol/l (n=256) (Hvas, 2001a).
The Danish researchers then studied a subset of 140 subjects with MMA levels of 400 to 2,000 nmol/l. The average age was 75 and participants had normal kidney function. After receiving B12 injections there were no improvements in a wide range of neurological symptoms (Hvas, 2001b) and depression (Hvas, 2004), and there was an improvement in only 1 of 8 measures of quality of life (Hvas, 2003) in comparison to the placebo group. However, a subgroup analysis of only those with baseline MMA levels of >600 nmol/l showed some improvement in neurological symptoms (Hvas, 2001b).
In a case series study from New York of people with overt neurological symptoms from B12 malabsorption, MMA levels ranged from 755 to 187,000 nmol/l (Lindenbaum, 1988).
Genetic polymorphisms may be a contributing factor as to why it’s hard to precisely pin down a healthy MMA threshold. In two ethnically Irish populations, one of young adults and another of adults ≥60, two different polymorphisms were found to increase MMA levels. For the adults ≥60, the people who were homozygous for one of the polymorphisms (31% of the population studied) had average MMA levels of 420 nmol/l. These polymorphisms are unrelated to cobalamin metabolism and the elevated MMA levels do not, by themselves, indicate a B12 deficiency (Molloy, 2016).
Methylmalonic Acid Levels among Older Adults
Older adults appear to have higher average MMA levels without apparent consequence.
A study from the Netherlands set reference intervals at 100–400 nmol/l for adults age 18–64 and 120–460 nmol/l for adults ≥65 (Abildgaard, 2021). These numbers were based on 95% confidence intervals of MMA levels among apparently healthy people with normal serum B12 and kidney function.
An analysis of the U.S. National Health and Nutrition Examination Survey data found that the normal serum MMA range for the 2.5th to 97.5th percentile of people ≥70 years, who were considered to be vitamin B12-replete and with normal kidney function, was 84 to 317 nmol/l (Mineva, 2019).
A study from Norway found the 2.5th to 97.5th percentile among people aged 71 to 74 to be 100 to 360 nmol/l (Vogiatzoglou, 2009). A study from the Netherlands found the 25th to 75th percentile among people ≥65 to be 180 to 300 nmol/l (van Wijngaarden, 2017).
A cross-sectional report from the Oxford Aging Project found that the 80th percentile for MMA was 350 nmol/l among people age ≥65 years (Clarke, 2003). The researchers believed an MMA level of ≥350 nmol/l could be indicative of a functional B12 deficiency. In contrast, the EFSA reports that a cut-off value of 750 nmol/l is used for the diagnosis of cobalamin deficiency for all ages (EFSA, 2015).
A study from The Netherlands (Riphagen, 2020) found that after 8.5 years of follow-up of an older cohort (median baseline age=65), a doubling of baseline MMA levels was associated with an increased risk of mortality (HR 11.48, CI 3.32–39.64). However, only 22% of the variation in MMA levels was explained by vitamin B12, estimated glomerular filtration rate, age, sex, and socioeconomic status, suggesting that other underlying disease was likely the reason for elevated MMA levels.
Studies treating mild to moderate B12 deficiency in older people have failed to provide cognitive benefits:
- A clinical trial from the Netherlands measured the cognitive response to B12 supplements in people ≥70 years old with mild B12 deficiency and MMA levels ≥320 nmol/l (average: ~450 nmol/l). The treatment was 1,000 µg of cyanocobalamin (n=54), 1,000 µg of cyanocobalamin plus 400 µg of folate (n=51), and a placebo (n=57). After 24 weeks, Mini-Mental State Examination (MMSE) scores didn’t significantly improve in the treatment groups compared to the placebo, and the placebo group actually improved significantly more than the B12-only group (Eussen, 2006).
- A clinical trial from the UK measured cognitive or other neurological functions in response to B12 supplements in 191 asymptomatic, non-anemic older people with low B12 levels and considered moderately deficient. The treatment was 1,000 µg/day of cyanocobalamin. After one year, there was no evidence of any benefit on a wide range of cognitive and physical outcomes. MMA levels weren’t measured (Dangour, 2015).
- A clinical trial from Australia measured MMSE scores in response to B12 supplements in 20 adults aged 82 to 85 with low B12 levels (about 150 pmol/l). The treatment was 10 µg or 50 µg of B12 daily. After 4 weeks, the treatment group’s MMSE scores didn’t improve more from baseline than did the placebo group’s. MMA levels weren’t measured (Seal, 2000).
To summarize, there’s a lack of evidence that striving to minimize MMA levels beyond what’s normal for one’s age group has any tangible cognitive benefits.
Appendix B. Clinical Trials: Impact of B12 Supplementation on Metabolites
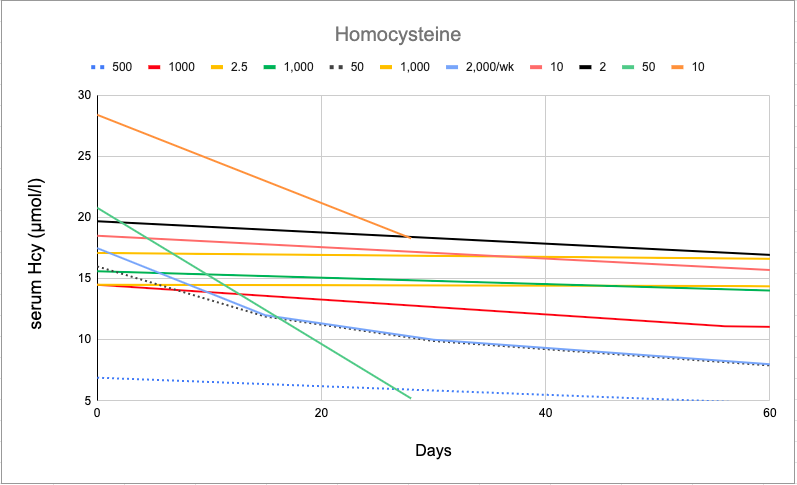
Below are four graphs showing the response to B12 supplementation of serum B12, holotranscobalamin, MMA, and homocysteine:
- Eight trials of predominantly older adults with at least mild deficiency (Dangour, 2015; Eussen, 2005; Eussen, 2006; Hill, 2013; Kuzminski, 1998; Rajan, 2002; Seal, 2000; Verhaeverbeke, 1997)
- One trial of predominantly vegetarian families from India (Deshmukh, 2010)
- One trial of half vegetarians and half vegans whose responses were mixed together (Del Bo, 2019)
- One trial of B12 supplementation in vegans who weren’t previously supplementing (Crane, 1998)
The dotted lines represent the trial of only vegans (500 µg per day by Crane et al.) and the trial of half vegetarians and half vegans (50 µg and 2,000/wk by Del Bo, 2019). You can match the dosage legend (across the top from left to right) with the lines starting from bottom to top.
Serum B12
The graphs show a general trend of quick, initial changes which then slow over time, and that the poorer your initial B12 status is, the more quickly it initially changes. Even the smallest doses seem to have an impact.
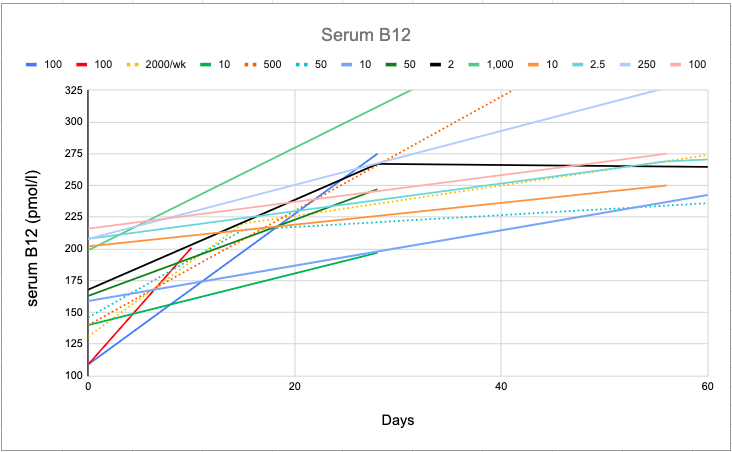
For reference, a serum B12 of <148 pmol/l has commonly been used to determine B12 deficiency, and has shown good sensitivity (95 to 97%; specificity <80%) for the diagnosis of deficiency in patients with megaloblastic anaemia or neurological abnormalities (EFSA, 2015).
Holotranscobalamin
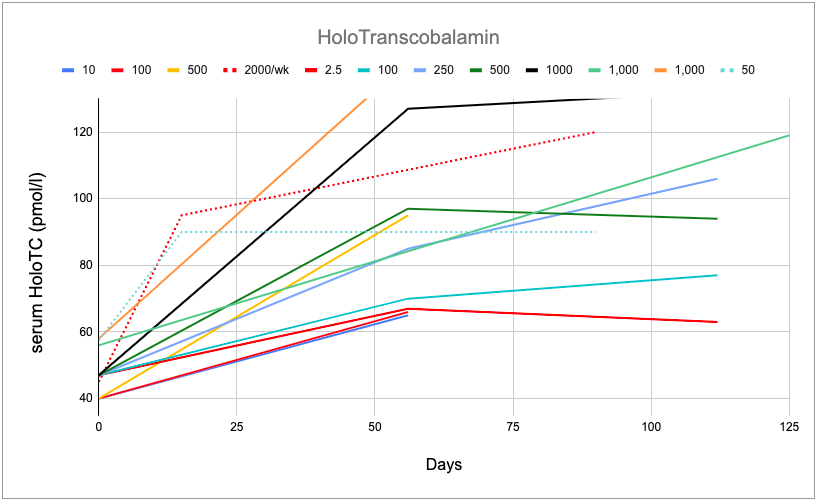
Holotranscobalamin is the fraction of serum B12 that is attached to the B12-transport protein transcobalamin and is considered the physiologically active form because it delivers B12 to the cells for utilization.
Holotranscobalamin normally makes up 10-30% of the B12 in healthy people (EFSA, 2015). With supplementation, holotranscobalamin increases proportionally to serum B12.
Some researchers have argued that holotranscobalamin is a better measure of B12 deficiency than total serum B12 due to holotranscobalamin’s relatively short half-life. Lloyd-Wright et al. (2003) suggest that holotranscobalamin can be a particularly useful test for vegans such that >50 pmol/l indicates B12 sufficiency, 25 to 50 pmol/l indicates a need for testing other biomarkers, and < 25 pmol/l indicates B12 deficiency.
Golding points out that unless the enterohepatic circulation is disrupted, holotranscobalamin levels won’t significantly decrease until the liver’s B12 stores are depleted (Golding, 2016). In pernicious anemia, holotranscobalamin decreases whereas in dietary deficiency, holotranscobalamin will remain relatively stable while total serum B12 decreases.
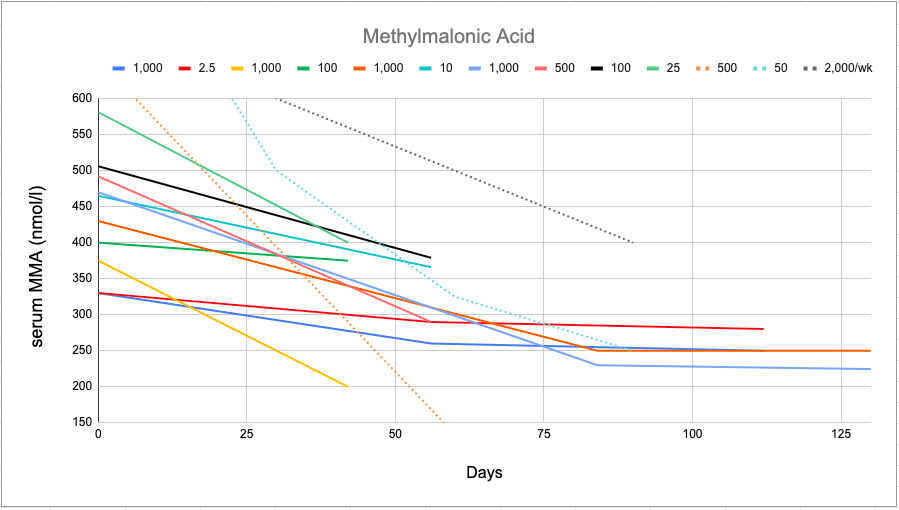
Methylmalonic Acid
Homocysteine
Notes on Clinical Trials of B12 Supplementation
Although not addressed in the graphs, younger people who start out deficient tend to have more drastic, initial drops in MMA and homocysteine.
The data for these charts are located in the spreadsheet B12 Supplementation Trials where studies can be matched with the lines and additional doses are listed. Including all doses in the charts above would have made them unreadable so we eliminated similar dose-responses. Some studies didn’t report on all of the parameters and don’t appear in every chart.
Kuzminski et al. treated people suffering from severe B12 malabsorption with 2,000 µg of cyanocobalamin per day (Kuzminski, 1998). The details are included in B12 Supplementation Trials, but the baseline parameters were such outliers, and the response to treatment was so drastic, that the lines didn’t fit in the charts. Suffice it to say that a 2,000 µg/day dose of cyanocobalamin is enough to ensure maximum B12 status in anyone without an extremely rare condition.
The 500 µg per day study by Crane et al. was of two vegan families who had been vegan for at least two years and had not regularly received B12 from supplements or fortified foods (Crane, 1998). Only one vegan had clinical symptoms of B12 deficiency, mild numbness in one hand, which resolved upon supplementation.
A clinical trial from Spain treated adults, with an average age of 74, for eight weeks with 1,000 µg of cyanocobalamin per day and then for another 46 weeks with 1,000 µg per week. While the daily dose was sufficient to maintain serum B12 levels above 156 pmol/l in almost all subjects, the weekly dose was only able to do so in 74% of subjects (Sanz-Cuesta, 2020).
Extrapolating from B12 supplementation trials of non-vegans to determine the needs of vegans is complicated by the fact that a high percentage of any small dose of B12 is absorbed and omnivores are normally receiving numerous small doses throughout the day. In other words, we can’t directly extrapolate recommendations for vegans from the trials in the graphs above except to know that 500 µg per day is enough for vegans based on Crane, 1998.
In summary, cyanocobalamin supplementation, even at small doses, has a marked impact on the above blood parameters for the average person with either low B12 intakes or mild B12 malabsorption, including for older people.
Appendix C. Factorial Approach
Researchers have attempted to determine B12 needs by measuring daily B12 body losses, also known as the factorial approach.
A 2012 review of all known studies determined that daily B12 losses in apparently healthy adults and elderly range from 1.4 to 5.1 μg (Doets, 2012). The rate of loss is a fixed percentage of total body stores—the larger the body stores, the larger the absolute amount lost. They also found that lower body stores are correlated with higher absorption rates.
We’re more interested in body losses for people on the lower end of normal for total body stores, as there’s no need to replenish excess amounts. The most recent study on total B12 body count was also the study that found the lowest body stores (Bessent, 1980). They measured the full B12 body count of four people and found it to be 780 to 1,350 µg of B12 with a daily loss of 0.12% for a maximum loss of 1.6 µg per day or 11.2 µg per week.
In their review, Doets et al. noted that the research on body losses is relatively old, inconsistent, and it might not be further clarified due to the ethical concerns with using radioisotopes for tracking B12 in the body. The EFSA notes, “The inherent uncertainty of this [factorial] approach is reflected in the wide range of cobalamin intake calculated to compensate for estimated daily losses, depending on the assumptions taken (EFSA, 2015).”
Appendix D. Pregnancy and Breastfeeding
There’s some controversy about whether pregnant and breastfeeding women can maintain a healthy B12 status for themselves, their fetuses, or their infants without a daily B12 intake. There has been very little research to draw upon to answer this question.
In a report from the January 2020 workshop Nutrition During Pregnancy and Lactation, nutrition expert Dr. Lindsay Allen said that smaller, repeated doses of B12 during breastfeeding, rather than a single one-a-day supplement, appear to be more effective for the mother’s B12 status (NASEM, 2020). However, the report doesn’t provide any citations. We messaged the author in October of 2020 but haven’t heard back.
Passive absorption of B12 may be greater for pregnant women. B12 levels increased significantly more for pregnant than non-pregnant women when given an oral dose of 1,000 µg (respective increase of 195 vs 117 pmol/l) or 500 µg (respective increase of 147 vs 95 pmol/l), but not for 250 µg (respective increase of 11 vs. 35 pmol/l; Hellegers, 1957).
Giugliani et al. measured B12 levels in 51 mothers, placentas, and infants post-delivery, and found that the intervillous space in the placenta contained a higher concentration of B12 (796 pmol/l) than the blood of the mothers (590 pmol/l) or their newborns (252 pmol/l). They concluded that “B12 accumulation in the placenta may represent an important factor in providing sufficient amount of this essential nutrient to the fetus (Giugliani, 1985).”
Due to a lack of clinical trials and case reports examining non-daily doses of B12 in pregnant or breastfeeding women, perhaps non-daily injections can provide some insight.
Sixteen breastfeeding mothers suspected of B12 deficiency were given a B12 injection of 50 µg. There was a large increase in breast milk B12 that dropped to baseline levels over the course of 5 to 6 days. Breast milk concentration increased from an average of 55 pmol/l to about 1,000 pmol/l. Malabsorption didn’t appear to be a problem for the women who had very low animal product intake providing an estimated 0.5 to 2.0 µg of B12 per day. B12-deficiency symptoms in the infants improved (Srikantia, 1967). This study provides some confidence that B12 intake isn’t required on a daily basis for breastfeeding mothers, but a 50 µg injection represents about 4 times the weekly absorption our recommendations provide.
We found two other cases of injections being effective during pregnancy: 1,000 µg every two weeks and 5,000 µg per week (Vithlani, 2017).
Due to a lack of information and the importance of B12 for neurological development in the fetus and infants, we recommend daily supplementation during pregnancy and breastfeeding.
Appendix E. IOM Recommendations for People Over Age 50
The U.S. Institute of Medicine says, “Since 10-30% of older people may malabsorb food-bound B12, it is advisable for those older than 50 to meet their RDA mainly by consuming foods fortified with B12 or a B12-containing supplement (IOM, 1998, p. 306).” This is likely due to decreased digestive enzyme production or decreased stomach acid resulting in a decreased ability to cleave B12 from its carrier proteins in animal foods.
Appendix F. ASMBS B12 Recommendations for People after Bariatric Surgery
The American Society for Metabolic and Bariatric Surgery has B12 recommendations for patients after bariatric surgery (Parrott, 2017):
- 350 to 500 µg per day if taken orally.
- Routine screening of B12 status.
- If found deficient, 1,000 µg/day to achieve normal levels; then resume regular dosages.
These recommendations should be adequate for vegans post-bariatric surgery.
Appendix G: Taking Vitamin B12 With or Without Food
Stephen Walsh summarizes the evidence from four papers on B12 absorption (Doets, 2012; Berlin, 1968; Heyssel, 1966; Siegel, 1961):
Absorption tests with food, using a flushing vitamin B12 injection to estimate absorption, indicate a reduction of the passive absorption by about 40% when supplements are taken with food rather than when fasting. In contrast, there is some evidence of an enhancement of the maximum absorption via intrinsic factor, by up to a factor of 2, when the vitamin B12 is accompanied by food, but this is not consistently observed and probably only applies when the food quantity and vitamin B12 dose are sufficient to slow the passage of the vitamin B12 through the small intestine enough (about three hours or more) to allow each intrinsic factor receptor to absorb two molecules of vitamin B12 from the oral dose rather than one. Doses of above 400 micrograms are best taken on an empty stomach if one wants to maximise the absorbed amount. For lower doses it’s more uncertain but there is a potential benefit to taking them with food.
All of the vitamin B12 absorption calculations we use give doses that are sufficient regardless of whether food is consumed with the B12.
Bibliography
Berry CG. Anaemia of pregnancy in Africans of Lagos. Br Med J. 1955 Oct 1;2(4943):819-23. Not cited. Cobalamin injections of 200–250 µg/wk initially, followed by 50 µg/wk, alleviated the symptoms of anemia in women post-pregnancy.
Greibe E, Andreasen BH, Lildballe DL, Morkbak AL, Hvas AM, Nexo E. Uptake of cobalamin and markers of cobalamin status: a longitudinal study of healthy pregnant women. Clin Chem Lab Med. 2011 Nov;49(11):1877-82. Not cited. Greibe et al. compared B12 absorption throughout pregnancy (at 13, 24, and 36 weeks) and found no difference in absorption at those times.
Hoey H, Linnell JC, Oberholzer VG, Laurance BM. Vitamin B12 deficiency in a breastfed infant of a mother with pernicious anaemia. J R Soc Med. 1982 Aug;75(8):656-8. Not cited. A 14-month-old girl developed severe B12 deficiency. She had been exclusively breastfed due to not wanting solid foods. Mother turned out to have pernicious anemia with a serum B12 of 96 pmol/l.
Luhby AL, Cooperman JM, Donnenfeld AM, Herrero JM, Teller DN, Wenig JB. Observations on transfer of vitamin B12 from mother to fetus and newborn. Am J Dis Child. 1958;96:532–533. Not cited. This short report lacked details, including the amount of B12 provided to the mothers.
Stover PJ. Vitamin B12 and older adults. Curr Opin Clin Nutr Metab Care. 2010;13(1):24–27. Not cited.