Contents
- Summary
- Introduction
- Cyanide
- Effectiveness
- Absorption
- Methylcobalamin Trial in Vegans
- Cross-sectional Data from Romania
- Case Study from Germany
- Anecdotal Report from a Vegan
- Hydroxocobalamin
- Bibliography
Summary
Cyanocobalamin is a well-studied, reliable, inexpensive form of vitamin B12, though it does contain a molecule of cyanide, which, in normal amounts, should be physiologically inconsequential for most people. Many alternative health practitioners and supplement companies promote the coenzyme forms of B12, methylcobalamin and adenosylcobalamin. Requirements for these alternative forms have not been fully elucidated and common recommendations are for 1,000 µg/day.
Introduction
There are four forms of vitamin B12, differentiated by the side group attached to the cobalamin molecule:
- Adenosylcobalamin
- Cyanocobalamin
- Hydroxocobalamin
- Methylcobalamin
Methylcobalamin and adenosylcobalamin are the two forms of vitamin B12 that are coenzymes: the body requires each of them for different reactions.
Cyanocobalamin is the form most commonly found in supplements and fortified foods. It is the most stable because the side group, cyanide, has the strongest attraction to the cobalamin molecule.
Hydroxocobalamin is the form usually contained in B12 shots and the hydroxyl side group has the least attraction to the cobalamin molecule.
Adenosylcobalamin is technically 5′-deoxy-5′-adenosylcobalamin, and also known as dibencozide, cobamamide, and cobinamide.
The coenzyme form of B12 supplements, adenosylcobalamin and methylcobalamin, are sometimes promoted as being superior to cyanocobalamin for two reasons:
- Cyanocobalamin contains a molecule of cyanide.
- The body must convert cyanocobalamin into adenosylcobalamin and methylcobalamin before using it.
Others suggest that cyanocobalamin is the best choice for most people because it is the most stable form, it has been well studied and proven to increase vitamin B12 status, it is the most common, and least expensive.
Let’s examine the claims in favor of the coenzyme forms.
Cyanide
The safety of cyanocobalamin has raised concerns due to the fact that cyanide is a component of cyanocobalamin. The amount of cyanide in a cyanocobalamin supplement is a fraction of the amount of cyanide most people ingest on a daily basis and is considered to be physiologically insignificant.
For more information, see our detailed analysis in Vitamin B12 and Cyanide.
Effectiveness
Obeid et al. (2015) suggest that people do not benefit more from the coenzyme forms because all forms, except injected hydroxocobalamin, must have their side groups stripped by the target cell before the necessary side group is added for the coenzyme form needed. In other words, any form of cobalamin supplement can be turned into both of the coenzyme forms (methylcobalamin and adenosylcobalamin). They state:
Currently, we do not have sufficient evidence to suggest that the benefits of using [methylcobalamin] or [adenosylcobalamin] override that of using [cyanocobalamin] or [hydroxocobalamin] in terms of bioavailability, biochemical effects, or clinical efficacy. There is uncertainty regarding the claimed superior role of [B12] coenzyme forms for prevention and treatment of [B12] deficiency. However, [hydroxocobalamin] may be an advantageous precursor of the cofactors, particularly in the inherited disorders of metabolic [cobalamin] processing. [Cyanocobalamin] is a more stable and inexpensive form that appears to be best suited for oral supplementation and parenteral [intravenous] treatment as well.
People with genetic defects of vitamin B12 metabolism may benefit from hydroxocobalamin injections; Obeid et al. describe these genetic defects in more detail in their paper.
Absorption
Some researchers question whether the coenzyme supplements are stable in their oral form and usually recommend much higher doses of methylcobalamin—typically 1,000 µg/day.
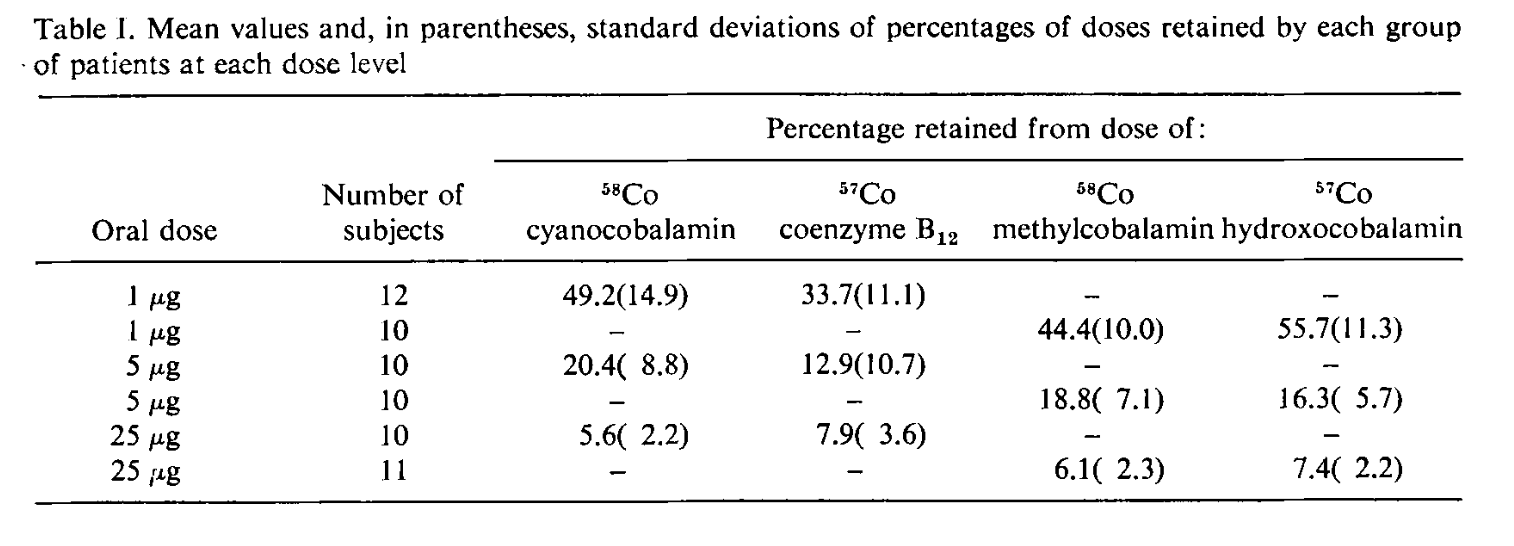
A 1971 study found that at doses of 1 µg, 5 µg, and 25 µg, cyanocobalamin, hydroxocobalamin, methylcobalamin, and adenosylcobalamin were all absorbed at about the same rate (Adams, 1971). Here’s a table of the absorption rates:
A 1973 study suggests that once absorbed, methylcobalamin may be retained in the body better than cyanocobalamin (Okuda, 1973).
A clinical trial from Korea found that 3 months of 1,500 µg/day of methylcobalamin raised B12 levels, reduced or eliminated neurological symptoms of B12 deficiency, and lowered homocysteine levels (Kim, 2011). This trial was done on people who had a gastrectomy and, therefore, had vitamin B12 malabsorption, indicating that for most people 1,500 µg/day would be more than enough. There was no comparison group receiving cyanocobalamin.
I am unaware of any clinical trials testing the various forms of vitamin B12 against each other among the general population and most people seem to do well using cyanocobalamin.
Some people with chronic fatigue report getting more relief from adenosylcobalamin than either methylcobalamin or cyanocobalamin (more info), while other people report feeling better only when taking both adenosylcobalamin and methylcobalamin. It’s possible this could be a real effect, but could also be due to a placebo effect or taking more B12 and inadvertently counteracting malabsorption.
Methylcobalamin Trial in Vegans
Donaldson (2000, USA) studied 3 vegans with elevated urinary MMA levels who were treated with 1/2 to 1 sublingual methylcobalamin tablet, 2 times/day for 3 weeks. Correspondence with the author (March 21, 2002) verified that these tablets contained 1,000 µg methylcobalamin each.
Two of the subjects’ urinary MMA normalized while the remaining subject’s stayed slightly elevated at 4.1 µg/mg creatinine (normal is < 4.0 µg/mg creatinine). Thus, at a rate of 1,000-2,000 µg/day, methylcobalamin appears to be absorbed at a high enough rate to improve B12 status in some vegans. Additionally, this indicates that the methylcobalamin was converted to adenosylcobalamin for use in the MMA pathway.
Cross-sectional Data from Romania
A cross-sectional study from Romania found that vegans supplementing with cyanocobalamin had higher levels of holotranscobalamin than those supplementing with methylcobalamin (150 pmol/l and 78.5 pmol/l, respectively; p-value=0.030; Zugrav et al, 2021). However, those taking methylcobalamin supplemented less and the amounts varied.
A holotranscobalamin level of 78.5 pmol/l is well above the minimum healthy range indicating that the methylcobalamin regimen was adequate. The average dose for those supplementing with cyanocobalamin and methylcobalamin was 582 µg and 988 µg, respectively. The frequency of methylcobalamin intake was 21% daily, 36% twice per week, and 43% once a week. Without assessing MMA levels and more precisely correlating values with intake amounts and frequency it’s not possible to determine a reliable regimen.
Case Study from Germany
Storz et al. (2024, Germany) reported a case study of one middle-aged man who had been taking a single oral dose of 500 µg of methylcobalamin and an average of 3 to 4 times a week for many years. His vitamin B12 levels were healthy at 303 pmol/l (409 pg/ml) and his homocysteine level was 11.7 µmol/l (above 12 µmol/l is considered unhealthy).
Anecdotal Report from a Vegan
In 2011, a reader sent in this report:
I’d been taking 500 µg of methylcobalamin for years, not knowing that the B12 dosages so often cited (daily 25 – 100 µg) are just for cyanocobalamin. So, about a week ago I started taking 1000-2000 µg of methylcobalamin instead of just 500 µg, and I feel a difference!
It should be noted that this person might suffer from B12 malabsorption of any form of B12, and might have had the same experience with cyanocobalamin.
Hydroxocobalamin
Hydroxocobalamin is the form of B12 typically found in food. There are not many oral forms for people to take; it is normally injected. One study suggests that after injections, hydroxocobalamin is retained in the body better than cyanocobalamin (Tudhope, 1967).
Bibliography
Chalmers JN, Shinton NK. Comparison of hydroxocobalamin and cyanocobalamin in the treatment of pernicious anaemia. Lancet. 1965 Dec 25;2(7426):1305-8. B12 administered by injection. Not cited.
Donaldson MS. Metabolic vitamin B12 status on a mostly raw vegan diet with follow-up using tablets, nutritional yeast, or probiotic supplements. Ann Nutr Metab. 2000;44(5-6):229-34. The subjects receiving methylcobalamin was only a small part of this paper, mentioned on p. 232.
Kelly G. The co-enzyme forms of vitamin B12: Toward an understanding of their therapeutic potential. Alt Med Rev. 1997;2(6):459-471. Not cited.
Okuda K, Yashima K, Kitazaki T, Takara I. Intestinal absorption and concurrent chemical changes of methylcobalamin. J Lab Clin Med. 1973 Apr;81(4):557-67.
Sawangjit R, Thongphui S, Chaichompu W, Phumart P. Efficacy and Safety of Mecobalamin on Peripheral Neuropathy: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. J Altern Complement Med. 2020 Dec;26(12):1117-1129. Concluded that mecobalamin (aka methylcobalamin) taken orally (1500 mg/day), intramuscularly, or intravenously (500 mg/day) may be effective for the treatment of diabetic neuropathy. Not cited.
Tudhope GR, Swan HT, Spray GH. Patient variation in pernicious anaemia, as shown in a clinical trial of cyanocobalamin, hydroxocobalamin and cyanocobalamin-zinc tannate. Br J Haematol. 1967 Mar;13(2):216-28.
22 thoughts on “Coenzyme Supplements: Methylcobalamin and Adenosylcobalamin”
Hi, it is very hard to find low doses of B12 for kids. And most cyanocobalamin come in lozenges which is hard for young kids. How much methylcobalamin should I give my kids? I was hoping to find here the same sheet you have for cyanocobalamin. Thank you!
Liz,
I wouldn’t know how much methylcobalamin to give kids—I’d figure out a way to stick to cyanocobalamin. Have you looked into fortified foods? Or you might try crushing a lozenge and sprinkle a little bit in their food each day.
Lisa, Nature’s Bounty 5000mcg B12 is made with cyanocobalamin. It’s available in grocery stores that sell vitamins and available in drug stores
Hello,
when I went vegan about 12 years ago, I read a lot about B12 and I found a very inexpensive and safe supplement method, using cyanocobalamin products. Now I just wanted to re-order one of these – but none is available anymore. When I search for “B12” at the German amazon or other websites, there is only methylcobalamin!
I think this might be a problem, if people look at the dosage recommendations that were developed in studies with cyanocobalamin.
Just wanted to share this thought… Hope there will be more studies with methylcobalamin, which is what I have to buy now. At a higher price, of course.
Best wishes to you!
Hello.
I am writing through a translator, I hope it will be clear what I have written.
Please tell me when you write at the beginning of the article that the general recommendations for taking methylcobalamin are considered to be 1000 mcg per day, do you approve of this recommendation, or are you just stating a fact?
can you advise vegans to take 1000 mcg per day if they do not have an increased need for vitamin and no malabsorption?
Marta,
Based on very limited data, it appears that vegans can take 1,000 µg per day of methylcobalamin and it should be enough to maintain healthy vitamin B12 status.
Hi, and thanks for the fantastic work you’re doing with this website!
I’m afraid however, that after reading this, the reasons why the recommended daily dose for methylcobalamine is so much higher than that for cyanocobalamine are still not entirely clear to me.
– “Some researchers question whether the co-enzyme supplements are stable in their oral form”: is this questioning based on experimental evidence, or are there other reasons to think those forms might be less stable?
– “Requirements for these alternative forms have not been fully elucidated”: some of the studies cited on this page seem to suggest that the alternative forms are well absorbed and well retained in the body. In your opinion, what’s missing to fully elucidate requirements for these alternative forms? Would other kinds of studies be needed (if so, what kind), or is just a matter larger sample sizes and/or a larger number of concordant studies by various teams?
Please don’t misinterpret my questions: I’m not trying to advocate for these alternative forms, I’m happily taking a cyanocobalamin supplement because I understand that’s the form backed by the most evidence so far (also, it’s the cheapest and even if there wasn’t questions about alternative forms, I wouldn’t see any reason to pay more). I’m just trying to understand the reasoning better.
Thanks again for the wealth of quality content on this site, and looking forward to reading your response!
Manuel,
Before recommending methyl or adenosyl, I would want a study that compares MMA levels before and after supplementing at a range of dosages to determine what amounts consistently reduce MMA levels in most people. I’m guessing dozens of people for each dosage would be required to reach statistical meaningfulness.
Dr Norris: Thanks for getting back. The wording of your clarification sounds perfect. Thanks for taking the time to make this change. I think this is closed. I will continue to look for an article that contradicts this or provides some explanation for my situation and if I find one, I will contact you. Norman
Dr Norris: Thanks for getting back. The paragraph under effectiveness says that the ligands must be removed as a first step and then the form needed (methyl or adenosyl) must be synthesized in a second step inside the cell. This implies (might be better to state this explicitly) that either the methyl form or the adenosyl form will work as a supplement and so either form is complete. This ref: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5312744/ has a nice picture of this. Unfortunately, this does not match what I am seeing.
.
Your reply also says that people involved in testing large dose cyanocobalamin supplements never (rarely) experience reactions to the cyanide. I wonder how old the people involved in the testing are ? I think the testers should be over 65 (better over 70) because this is the group that is most likely to need this large dose.
Norman,
I added this sentence to clarify it: “In other words, any form of cobalamin supplement can be turned into both of the co-enzyme forms (methylcobalamin and adenosylcobalamin).”
As I mentioned before, if you have reduced kidney function, that could, at least theoretically, result in an inability to utilize cyanocobalamin. Regularly smoking cigarettes could also lead to reduced cyanocobalamin utilization (though it’s rare).
Yes, many studies have been done on older people taking 1,000 µg of cyanocobalamin per day.
Dr Norris:
Thank you for taking the time to review my comment and prepare a response.
You are saying the average daily intake of cyanide from food is around 90 mcg whereas the amount of cyanide from 1/10 of a 1000 mcg cyanocobalamin tablet is 2 mcg.
This implies that if I felt sick from the cyanocobalamin tablet, then I should feel even more sick from the food I eat. The problem is that I don’t feel sick like that every day.
To investigate this, I could purchase another bottle of cyanocobalamin tablets and repeat the experiment. But if I did this and did experience the same feeling of being sick, I have no way to investigate to determine what is going on. So since I am happy with the current situation, I will let this one go.
It would be helpful if you could address my first question on your website. If methyl cobalamin is complete, it should say so. If it is not complete, it should say that taking both methy and adenosyl cobalamin is advised for complete B12 coverage. If it is unknown, then it should say this question is under investigation and taking both forms is advised until the research is completed.
Thank you again for your help with this.
Norman
My first question is whether methyl cobalamin is complete ? From my testing it appears it is not and I needed to add adenosyl cobalamin to fix. Regarding the safety of cyanocobalamin, at about 72 all of a sudden I started having symptoms of B12 deficiency. My intake of cyanocobalamin had not changed. I added a methyl cobalamin supplement and the symptoms were fixed. My conclusion is that I can no longer process cyanocobalamin into the active forms. I tried to find statistics on how many people hit this problem and could not find any. If significant numbers of people are going to lose the ability to process cyanocobalamin as part of the aging process, it would be good to make people aware of this instead of having each person puzzle it out on their own. It would be helpful if this article could address these 2 topics.
Norman,
It’s highly unlikely that you’ve lost the ability to convert cyanocobalamin to one of the co-enzyme forms. It’s not terribly unusual for people to lose the ability to absorb vitamin B12 as they age, but that would be true of all forms, not just cyanocobalamin.
If you’d like to provide your supplementation regimen and more details about why you think this is the case, I’m happy to give you my thoughts.
06/29/2020
Here are the steps I followed to investigate my B12 problem.
The problem popped up very quickly. Everything was fine and then over a couple of days I was experiencing tingling, burning, and numbness in my feet.
I am generally familiar with nutrient deficiency symptoms so I assumed it was a B12 problem.
1) I reviewed my intake of cyanocobalamin:
12.5 mcg from 1/2 Centrum multivitamin
(I assumed B12 coming in from the diet was 0)
This had not changed.
2) I decided to try a larger dose of cyanocobalamin. I purchased a bottle of the large tablets (I don’t have that product any more so I don’t recall the dose. Based on what products are available now I would say it was either 1000 or 1500 mcg). I cut off about 1/10 of the tablet and took it.
After some time (I think 30-60 minutes), I noticed that I felt sick and there was no impact on the tingling. From this, I concluded I could absorb it but I was not detoxifying the cyanide fast enough. So I decided to reject this option.
3) I decided to try methyl cobalamin. The tablet size is 2500 mcg. I cut off about 1/10 of this (250 mcg) and took it (1/10 is more than I need but it is the smallest cut I can make without specialized tools). This fixed the tingling fairly quickly and there was no sensation of being sick. So I decided to go with this option. I played with the dose and finally got to 1/10 tablet twice per day which I have continued to the present.
4) Eventually I got around to mentioning this issue to my doctor. She said she was familiar with this problem and she agreed that switching to methy cobalamin was the right solution.
5) Around that time, I ran a B12 blood test and an MMA test. Both tests were normal.
6) More recently, a problem with chemical sensitivity (triggering inflammation) was becoming more serious. I investigated this and found that it might be caused by an adenosyl cobalamin deficiency. I added 2000 mcg of adenosyl cobalamin to my regimen. This has made the chemical sensitivity problem much better.
7) Conclusions:
⦁ The B12 issues seem to be fixed.
⦁ It is difficult for me to believe that I am unique with these problems and no one else is experiencing them except me.
Norman,
Thank you for the detailed explanation and I’m glad you’re feeling better.
I recently reviewed the literature on cyanocobalamin and cyanide intakes.
I couldn’t find data on average cyanide intakes for the U.S. or Canada, but the average adult cyanide intake from food in Europe is 1.42 µg/kg of body weight per day. For a 140 lb (63.5 kg) person, that comes to 90 µg per day.
A 1,000 µg supplement of cyanocobalamin has 20 µg of cyanide. The acute reference dose (ARfD) for cyanide has been set at 20 µg/kg of body weight or 1,270 µg for a 140 lb person. That means a 140 lb person is receiving 1.6% of the ARfD for cyanide from a cyanocobalamin supplement versus 7.1% from food.
Unless someone has kidney impairment, this extra cyanide shouldn’t make a difference for B12 metabolism. While you might be an exception, the evidence favors the idea that people do not need to be concerned about cyanocobalamin in typical amounts.
I’ll look into the adenosylcobalamin and inflammation connection when I get a chance.
Actually it is very possible and has been reported before that some people seem to have trouble converting cyano to the active forms. Studies have found that methyl is best. Hydroxo next. Cyano is worst. The book Could it be b12? Is the most comprehensive I have found and goes into some detail about this.
Jay, if you can show us some peer-reviewed research in addition to what we’ve outlined above, I’d be happy to take a look at it to see if we should modify our view.
Dr Norris: One more point on this: I want to focus on this statement from my previous comment: “You are saying the average daily intake of cyanide from food is around 90 mcg whereas the amount of cyanide from 1/10 of a 1000 mcg cyanocobalamin tablet is 2 mcg.”
Looking at the total daily average of dietary cyanide intake is too high level. I can break that down to 30mcg from breakfast, 20mcg from lunch, and 40mcg from supper. I can assume these are cleared within 1 hour after the meal. I can conclude that if I ran the test immediately after dinner, my total exposure to cyanide would have been 42mcg. This is not enough of a difference (40 vs 42) to explain why I felt sick. So either there is something else in that tablet that made me sick, or your estimate of the amount of cyanide in 1/10 table is off by more than 40 times.
Norman,
> It would be helpful if you could address my first question on your website. If methyl cobalamin is complete, it should say so.
That’s what the section Effectiveness is intended to do.
> So either there is something else in that tablet that made me sick,
It’s possible you had a reaction to something else. We hear from people who say they have a reaction to high doses of cyanocobalamin. The odd thing is that there are never any such side effects mentioned in the B12 trials where many people are taking high doses.
Molecular weight of cyanocobalamin = 1355.38
Molecular weight of cyanide = 26.02 g/mol
26.02 / 1355.38 = 1.92%
1,000 µg * 1.92% = 19.2 µg
Any data on bioaccumulation of cyanide in tissues over the period of time ie from its continuous use?
Satendra,
I didn’t see any when I researched this article, but it’s not surprising given what a small amount of cyanide a cyanocobalamin supplement would contribute to the body—researchers probably wouldn’t consider it worth their time to investigate.